The SALG Patient Safety Updates contain important learning from incidents reported to the Learning From Patient Safety Events (LFPSE) system. The RCoA and the Association aim to bring these Safety Updates to the attention of as many anaesthetists and their teams as possible. The updates are published every four months and contain data from an earlier time period.
SALG Updates
SALG Patient Safety Conference: 21st October, 2026 – open for booking
The SALG Patient Safety Conference will be held virtually this year on Wednesday, 21st October, 2026.
The conference will focus on paediatric anaesthesia safety, with a programme developed in partnership with the Association of Paediatric Anaesthetists of Great Britain and Ireland.
Please book your place here
Resident anaesthetists are invited to submit abstracts describing projects or initiatives focusing on paediatric anaesthesia safety that measurably reduce harm, improve care processes and strengthen a culture of safety. The submissions will undergo review, and the highest scoring abstracts will be invited to present their work as either an oral presentation or an ePoster. Further details can be found on the conference booking page linked above.
Update on penicillamine/penicillin allergy recording
SALG identified this national patient safety risk after a member of our network reported an anomaly in their own trust’s electronic prescribing system and uncovered a potential nationwide issue. SALG alerted NHS England who are working with colleagues in Scotland to address the problem.
The issue involves patients’ penicillin allergy being incorrectly recorded as penicillamine allergy, that can and has led to administration of penicillin-type antibiotics to sensitive patients, resulting in anaphylactic reactions. A review of national incident data revealed 315 related reports over three years, including one fatality. This error can be propagated across care settings through shared records. An alert, issued by NHS England in December 2025 called for healthcare organisations to urgently review and correct allergy records, update training on EPS and work with system suppliers to implement safeguards.
HSSIB reports on safety of frontline digital systems
HSSIB have published a thematic review of patient safety issues related to electronic patient records (EPR), including electronic prescribing. The findings of this report are intended for those responsible for procuring, configuring, integrating and optimising EPR systems in healthcare at national, regional and local levels. HSSIB have also recently published a fourth investigation report on medication-related harm, which further highlights risks associated with digital systems and prescribing processes. Both reports are shared for the purposes of awareness.
Prevention of Future Deaths Reports
Paragraph 7 of Schedule 5, Coroners and Justice Act 2009, provides coroners with the duty to make reports to a person, organisation, local authority or government department or agency where the coroner believes that action should be taken to prevent future deaths. When a report is received by the Royal College of Anaesthetists or the Association of Anaesthetists, SALG submits a response and undertakes the appropriate patient safety initiatives.
We extend our deepest sympathy to the families of William King and Chloe Ulett, who are the subjects of the reports below.
Mr William (Billy) King
A prevention of future deaths report was received in September 2025 regarding the death of Mr William (Billy) King. The Coroner raised concerns about the process and documentation of consent discussions for nasogastric (NG) tube insertion prior to an emergency laparotomy for bowel obstruction. In response SALG highlights the following:
- The Association of Anaesthetists are in the process of updating their consent guidelines, endorsed by RCoA, and these will emphasise the need for discussions to occur prior to patients coming to the anaesthetic room. This is to ensure patients have the time and space to consider the risks and benefits of the options available and the anaesthetist’s recommended course of action.1
- A discussion between the anaesthetist and a patient regarding the risks/benefits of the anaesthetic should take place as soon as practicable after the decision to list a patient for emergency surgery is made.
- Documentation of this discussion should include the risks, benefits and alternatives discussed. Discussions around treatments that the patient refuses should be documented in as much detail as those they consent to.
Reference:
- Consent guidelines (In Press). Anaesthesia.
Miss Chloe Ulett
Following a coroner’s investigations into the death of Miss Ulett, a prevention of future deaths report was circulated to a number of Royal Colleges, including the Faculty of Intensive Care Medicine (FICM) in February 2026.
Three days after giving birth, Miss Ulett became acutely drowsy and confused with a reduced GCS. Her condition progressed rapidly within 24 hours to the point where she was unable to speak or move her arms and legs. A wide range of acute neurological conditions were considered, including encephalitis, meningitis and cerebral venous sinus thrombosis. She was found to have raised ammonia levels 3 days after admission, secondary to n-acetyl glutamate synthase deficiency, a Urea Cycle Disorder. By this time, it was too late for ammonia scavenging medications and haemofiltration to be effective and she had developed terminal cerebral oedema.
The Coroner was concerned about the delays to diagnosis and lack of early ammonia testing. The original report is available here. FICM’s response will be published in their next edition of their safety bulletin.
SALG considers it worth noting for all of those involved in the management of the obstetric population that any change in Glasgow Coma Scale (GCS) in a pregnant or recently pregnant patient should be considered a red flag. This principle is clearly stated in Royal College of Obstetricians and Gynaecologists (RCOG) guidelines on the management of the acutely ill pregnant woman,1 and it is also emphasised in the Managing Medical and Obstetric Emergencies and Trauma (mMOET) course2. In such situations, the patient should be admitted for urgent assessment and prompt investigation to identify the underlying cause.
It is possible that symptoms such as those exhibited by Miss Ulett were thought to be ‘normal for pregnancy’, a not uncommon reason for red flag symptoms to be missed, especially in settings where pregnant women are rarely encountered.
References:
- Royal College of Anaesthetists. Care of the critically ill woman in childbirth; enhanced maternal care. 2018
- Burns R, Dent K (eds.) Managing medical and obstetric emergencies and trauma: a practical approach. John Wiley & Sons; 2022
Safe Drug Management in Anaesthetic Practice Guidance, 2026
The Royal College of Anaesthetists and Association of Anaesthetists have reviewed and updated the safe drug management in anaesthetic practice’ guidance, and this was published on the SALG website in January.
The working party was chaired by Dr Naginder Singh, a former SALG scholar and current member of SALG. The guidance has been endorsed by the Royal Pharmaceutical Society and the College of Operating Department Practitioners.
Letter warning of fatal risks of wrong-route administration of tranexamic acid (TXA) published
The trade association, Medicines UK, published a letter on the 30th April, 2026 on behalf of marketing authorisation holders for TXA preparations, in agreement with the Medicines and Healthcare products Regulatory Agency. The letter highlights serious and fatal adverse reactions following inadvertent administration of tranexamic acid instead of local anaesthetics and advocates ‘extreme caution’ in storing, handling and administering intravenous formulations of tranexamic acid, including clearly labelling syringes containing tranexamic acid ‘for intravenous use only’ and storing tranexamic acid injectables separately from injectable local anaesthetics’.
In commenting on the letter, the Royal College of Anaesthetists’ President, Claire Shannon, said: ‘Our guidance on safe drug management is clear that all local anaesthetic solutions should be stored separately from IV infusion solutions, to reduce the risk of accidental IV or epidural administration. Prefilled syringes have also been shown to reduce medication errors, and our Safe Anaesthesia Liaison Group therefore advocates for more drugs to be made available in prefilled syringes, including tranexamic acid’.
SALG is continuing to work with manufacturers, both directly and via relevant trade association groups, to advocate for wider availability of prefilled syringes. This is particularly important for medicines such as tranexamic acid and local anaesthetics, where prefilled products can provide a physical safeguard against wrong-route medication errors. Regarding tranexamic acid, the adoption of pre-filled luer connector syringes, coupled with wide adoption of NRFit connector systems would significantly reduce the potential for human error causing significant harm or death.
Increased risk of anaesthetic neurotoxicity in patients of Venezuelan ancestry
SALG has been made aware of a recent alert by the American Society of Anaesthesiologists that people of Venezuelan heritage may be susceptible to anaesthetic neurotoxicity due to a mutation in their mitochondrial DNA (specifically, mtND4 m.11232T>C). This mutation is rare in this population, but it has resulted in unexpected catastrophic outcomes after routine anaesthesia in adult and paediatric patients reported by South American anaesthesia societies.
Whilst mitochondrial DNA is of maternal lineage, a negative family history of anaesthetic complications does not exclude this condition. The ASA recommends screening all patients with direct maternal Venezuelan lineage. This will necessitate directly questioning patients as Venezuelan lineage cannot be deduced from names, or routine ethnicity questionnaires. The number of people of Venezuelan descent living in the UK is unknown, as this is not recorded in official data as a separate category, but estimates range between 9,000 and 25,000 depending on the source.
There is no current point of care testing available for this specific mutation, and results can take up to 6 weeks to be returned. When ordering an EDTA test, anaesthetists should specify screening for the specific ND4 mutation when completing the form along with a 10ml blood sample.
Advice on clinical management, which is broadly relevant to UK settings, is included in the alert linked above, and replicated below for ease of reference:
The urgency of the procedure should inform the decision to proceed with the anaesthetic.
In the absence of definitive genetic testing, if the decision is made to proceed with anaesthesia and the patient is considered to be at risk, the anaesthetic plan should be developed considering the following:
- The optimal and safest anaesthetic for patients with this ND4 mutation has not been established.
- Given the majority of affected patients are reported to have received sevoflurane, consider avoiding the use of all volatile anaesthetics until more information is available.
- Regional anaesthesia should be considered for appropriate patients and procedures.
- Based on verbal reports, patients who have had complications from sevoflurane-based anaesthetics have had uneventful propofol anaesthetics. It is not yet known whether prolonged use of propofol infusions is safe in this population.
- Midazolam, dexmedetomidine, ketamine, and short/ultra-short-acting opioids have not been implicated.
- Anaesthetic depth monitoring with processed EEG to avoid burst suppression may be advisable. Some patients with complex I gene mutations show a rapid change (decrease) in EEG activity with exposure to volatile anaesthetics. It is unknown, at this time, if this rapid change is seen in patients of Venezuelan ancestry with the mutation.
- Patients at risk should be monitored after general anaesthesia for return to their neurocognitive baseline. Consider extended postoperative observation and monitoring of acid-base status if complications are suspected.
If similar complications to those described in the alert are observed in any patient, they should be reported through local risk management systems.
Wrong drug error – Adrenaline and Ephedrine
SALG were contacted by one of our regional leads about two incidents in which pre-filled adrenaline and ephedrine syringes were mistaken for one another. The similarity of the labelling on the syringes, due to identical colour schemes, was raised as a concern. SALG raised this with the syringe manufacturer, who explained that adrenaline syringes are intended to be differentiated by an additional outer wrapper (a lilac foil), unlike ephedrine and other pre-filled vasoconstrictors, which are supplied in blisters only. In these incidents, the outer wrapper appears to have been removed before the syringes reached the anaesthetist.
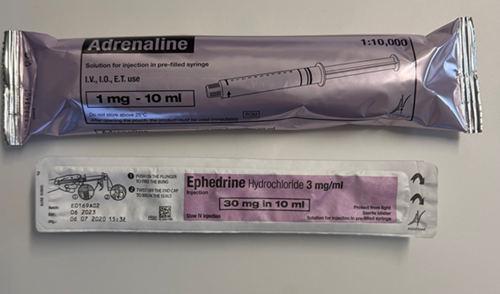


The colour scheme used on both the outer packaging and the syringe labels complies with BS ISO 26825:2020, which assigns colours based on anaesthetic drug class. This approach reflects the (generally) greater risk of harm from errors involving different drug classes. Adrenaline is a recognised exception to this, which is why this manufacturer added a distinctive outer wrapper, and why SALG recommends (below) keeping pre-filled syringes in all their packaging until use.
SALG considers the learning from these cases to include:
- The outer packaging (foil wrapper, blister or plastic cases) should never be removed from pre-filled syringes until immediately before administration. In the event that the outer packaging is removed from a pre-filled adrenaline syringe, but the syringe is unused, the syringe should be disposed of and not replaced in the cupboard for later use.
- All unused drugs (this includes ampoules, pre-filled syringes that are not in their original packaging and syringes that have been pre-drawn) should be removed from theatre/bench space and disposed of at an appropriate time. This should be either at the end of each case, or at the end of each theatre day, based on a risk assessment.
- There should be designated space in a cupboard/trolley/sealed container for drugs such as adrenaline that may be required in an emergency but are not routinely / frequently used.
- All members of staff who may be required to find/prepare/administer drugs such as adrenaline in an emergency should be familiar with:
- The location of emergency drugs
- The requirement to keep the drugs in their outer packaging until just before administration
- How the different drugs are packaged, including outer wrapping, the need to twist the top off pre-filled syringes and the dosage/concentration.
- It is an integral requirement to ensure patient safety that the labels on ampoules and syringes – whether these be pre-filled or pre-drawn - are actively checked before they are drawn up/administered to the patient. Syringes should be labelled, workspace should be organised and drugs checked by a second person where possible.1,2
References
1. Royal College of Anaesthetists. Safe drug management in anaesthetic practice. January, 2026
2. Association of Anaesthetists. Handling injectable medications in anaesthesia. Guidelines from the Association of Anaesthetists. June, 2023
Misplaced CVC line
This case was reported directly to SALG by an anaesthetist at the hospital where the incident occurred
A young adult admitted for orthopaedic surgery suddenly became unwell in theatre and was treated for suspected anaphylaxis to teicoplanin. Due to persistent hypotension, despite adrenaline via a peripheral line, an ultrasound guided right internal jugular central line was inserted, using a needle to identify the vein through which the guidewire was passed. The line was used for inotropes/vasopressors in theatre and ITU, and haemodynamic stability returned over a matter of hours.
Unfortunately, the patient didn't wake up when sedation was halted, and a CT head demonstrated widespread infarction. When the CVC inserted in theatre was transduced approximately 48 hours after insertion, there was an arterial trace (carotid). The patient was subsequently confirmed dead by neurological criteria and went on to organ donation.
There are several reports of such outcomes following inadvertent insertion and use of malpositioned CVCs, and FICM guidance emphasises the importance of transducing CVCs as soon as possible to exclude arterial placement. The key learning for our department is to 'transduce before use' and to re-establish continuous CVC monitoring despite its limited role in preload assessment.
Commentary:
The use of ultrasound does not guarantee correct placement of CVC. In haemodynamically compromised patients, arteries and veins may be hard to distinguish on ultrasound. The vein may be transfixed by the needle/ guidewire which subsequently end up in the artery. Consideration should be given to using a cannula to facilitate transduction and exclude arterial placement before dilatation, which even in the absence of infusions/ drugs can lead to catastrophic sequelae. The use of checklists is recommended, especially in emergency situations. Recent guidance has been published on Safe Vascular Access by the Association of Anaesthetists.1
The perioperative allergy network have also commented on the perioperative allergy aspect of this case:
Profound persistent hypotension with evidence of mast cell mobilisation is consistent with anaphylaxis, although differential diagnoses should be considered. Initial treatment with peripheral intravenous adrenaline, with placement of a central venous catheter (CVC) in the context of refractory anaphylaxis aligns with the RCUK perioperative anaphylaxis guidance.2.
Reference:
- Johnston AJ, Simpson MJ, McCormack V, Barton A, et al. Association of Anaesthetists guidelines: safe vascular access 2025. Anaes 2025; 80: 1381-1396. https://doi.org/10.1111/anae.16727
- Dodd et al. Emergency treatment of peri-operative anaphylaxis: Resuscitation Council UK algorithm for anaesthetist. Anaesthesia 2024, 79, 535–541. https://doi.org/10.1111/anae.16206
Review of clinical incidents
Following are reviews of incidents reported to the NHS in England and Wales in the period from 1st March – 30th June, 2025
Airway management
This content has been generated for SALG by Dr Sandeep Sudan on behalf of the Difficult Airway Society
A patient of short stature, with a history of vocal cord palsy (with no shortness of breath or stridor), was scheduled for a renal transplant.. On laryngoscopy, the vocal cords were adducted. Two unsuccessful attempts were made to intubate the trachea using a size 6 tube. A third attempt using a size 5 tube was also unsuccessful. The patient became impossible to ventilate or oxygenate and began to desaturate. Attempts to gain front-of-neck access were also unsuccessful. Eventually, oral intubation using a size 6 tube was achieved. A tracheostomy was performed by ENT, and the transplant procedure was abandoned.
Perioperative allergic reactions
This content has been generated for SALG by Dr Amy Dodd and Dr Linda Nel on behalf of the Perioperative Allergy Network
CASE 1
The patient undergoing a kidney transplant was given co-amoxiclav approximately an hour after induction of anaesthesia. Within 2 to 4 minutes intra-arterial monitoring revealed profound hypotension. The patient had been haemodynamically stable without vasopressor support prior to this event. Anaphylaxis was suspected and treated with 100 mcg adrenaline administered IV peripherally, with the patient head-down. Initially, there was no rash or angioedema, but a sparse urticarial rash was later noted on the abdomen.
Following discussion between anaesthetic and surgical consultants, after 15–20 minutes of stability, surgery continued. A sample was obtained for serum tryptase, and the reaction was documented in the electronic record. The patient was monitored postoperatively in the critical care unit for less than 24 hours before stepping down.
CASE 2
The patient experienced severe anaphylactic reaction possibly related to teicoplanin (previously tolerated without incident) during general anaesthesia in a standalone treatment centre. Despite treatment with adrenaline, steroids, nebulisers, and oxygen, the patient suffered a period of hypoxia and hypotension. The patient was transferred to ICU, where fluid resuscitation, adrenaline, advanced ventilatory support, and nebulisers continued. Tryptase blood samples were taken.
CT brain later showed cerebral oedema due to hypoxic brain injury, which progressed to clinical evidence of brain stem death and formal brain stem testing.
CASE 3
During induction of anaesthesia for a knee arthroscopy, severe bronchospasm after administration of fentanyl, propofol, and rocuronium raised the suspicion of anaphylaxis. Despite administration of adrenaline, ketamine, aminophylline, salbutamol, and hydrocortisone, the patient remained in severe bronchospasm for several hours and required transfer to intensive care intubated. Extubation was achieved the following day.
CASE 4
The patient suffered a cardiac arrest shortly after induction of anaesthesia for elective subacromial decompression. A straightforward nerve block had been performed, followed 10 minutes later by general anaesthesia. Whilst in the anaesthetic room, the patient suddenly developed bronchospasm. Prolonged resuscitation followed, including CPR and use of a LUCAS device. Inotropic support was required, including adrenaline and dopamine. Intralipid was administered
The patient was stabilised sufficiently for transfer to ICU. Despite maximal support over the next 24 hours the patient deteriorated, and life-sustaining treatment was withdrawn.
Differential diagnoses include anaphylaxis (serum tryptase later returned at 30.7), local anaesthetic toxicity, and tension pneumothorax (although chest drain insertion showed no evidence of tension). This case will be referred directly to the Coroner and a post-mortem is anticipated.
Aspiration
CASE 1
A Patient scheduled for emergency surgery, aspirated on induction. The patient was turned to the lateral position, the airway was suctioned, cricoid pressure applied and the trachea was intubated followed by fibreoptic bronchoscopy and removal of vomit from airways. The patient was transferred to critical care intubated and ventilated.
CASE 2
A frail patient with gastric outflow obstruction due to metastatic gastric cancer was scheduled for duodenal stent placement under sedation in interventional radiology. The patient had been on a liquid diet, had not vomited recently, did not have a nasogastric tube, and had fasted overnight. The risk of aspiration had been discussed during the team brief and sign-in. The left lateral position and use of endoscopic suction were used to mitigate this risk, but a decision was made not to intubate. Sedation was induced uneventfully, with spontaneous ventilation maintained throughout. The endoscopy revealed cancer and an empty stomach. After five minutes, brown liquid with particulate matter was noted in the mouth and on the pillow, without active vomiting. Endoscopic suction was ineffective. The oropharynx was suctioned, and further brown fluid was observed. The procedure was abandoned, and the breathing circuit on the anaesthetic machine was used to deliver oxygen. Although respiratory effort was maintained, oxygen saturation fell and the CO₂ trace became obtunded. An anaesthetic emergency call was put out. Respirations were assisted with face mask and PEEP, but there was no improvement in oxygen saturations or CO₂. Cardiac arrest was confirmed. Spontaneous circulation returned after 2 cycles of CPR and intubation of the trachea. Bronchoscopy confirmed material in the left lung. It is suspected that passing the endoscope beyond the cancer released unexpected distal fluid, which was then aspirated and caused a hypoxic arrest.
DNAR orders and iatrogenic cardiac arrest
CASE 1
Whilst waiting for a spinal block to develop the patient began coughing but remained cardiovascularly stable. Treatment for anaphylaxis followed advanced life support guidelines, and assistance was sought via the emergency buzzer. The patient become unresponsive and cardiac arrest was confirmed. A decision was made to stop resuscitation after two cycles as the patient was not for cardiopulmonary resuscitation and no reversible causes were identified. Death was confirmed.
CASE 2
The patient passed away in theatre following surgery, still intubated. A Consultant Anaesthetist, another anaesthetist, and an anaesthetic nurse were present. A DNACPR was in place for the patient and had been discussed and agreed during the team brief. No CPR was performed, as the plan was to provide reversible treatment only.
CASE 3
A patient, in their late 90s, underwent a six-hour intramedullary nail procedure. They had extensive comorbidities including bowel cancer (elected not for intervention), a clinical frailty score of 7 and a DNACPR for ward-level care. The patient could only mobilise with a walking frame and required assistance for personal care.
On arrival in recovery, the patient had a Glasgow coma score of 14, and an infusion of metaraminol had to be increased to support the BP. A few moments after being given a 50mcg bolus of fentanyl the low oxygen saturation alarm sounded, the saturation trace was lost and arterial trace became obtunded. A central pulse was present. The patient became bradycardic, then transiently asystolic, before ROSC with persisting bradycardia. Despite DNACPR it was decided this was a reversible medication-related event. The patient received 400 mcg naloxone, 200 mcg adrenaline, and oxygen via a Waters circuit. The patient rapidly started self-ventilating with a heart rate of 70–90 bpm.
Communication between anaesthesia and other members of the multidisciplinary team
CASE 1
A patient had a persistently low systolic BP in Recovery despite fluid resuscitation. The patient required oxygen and eventually was transferred overnight to HDU. The Recovery nurse felt their concerns about the patient, expressed to several anaesthetists, had not been adequately responded to.
CASE 2
The patient arrived in Recovery from Theatre with a metaraminol infusion at a rate that exceeded the locally prescribed maximum.
Approximately an hour later, the patient deteriorated, with an unrecordable blood pressure and hypoxia. An anaesthetist reviewed the patient, increased the metaraminol infusion and gave a bolus of adrenaline. 2 units red cells were transfused. After further reviews, a CVP line was inserted, and noradrenaline infusion started. The Recovery staff felt that if a CVP line had been sited and noradrenaline started earlier the collapse in Recovery could have been avoided.
Communication – Anaesthetists and surgical team
An elderly patient was listed for laparoscopic sigmoid colectomy After spinal anaesthesia was administered, the patient became profoundly hypotensive, and CPR was undertaken for a short period before induction of general anaesthesia. The surgical team were not informed of this episode at the time, and it was felt that the opportunity to discuss whether to continue with surgery had been missed, given the potential complications of chest compressions in a frail elderly patient with co-morbidities.
Postoperative prescribing/postoperative communication
CASE 1
Following surgery, several prescribed insulin doses were missed, resulting in the development of diabetic ketoacidosis. The patient subsequently suffered a cardiac arrest, was transferred to ITU and later died.
CASE 2
A patient suffering end stage liver failure underwent emergency gastroscopy for upper gastrointestinal bleeding in the early hours of the morning. At the time, the patient was significantly acidotic. Post-procedure, the patient was transferred to recovery as ICU-level care was deemed inappropriate.
Later that morning the patient began fitting and subsequently suffered a cardiac arrest. The recovery nurse reported shortly beforehand the patient had been speaking to family on the phone but had a low NEWS score, and had appeared mottled with a capillary refill time of 10 seconds. ABG taken at this time showed glucose <1 mmol/L and pH 6.5.
Lorazepam was administered for seizures. Return of spontaneous circulation was achieved after one cycle of CPR but the patient remained unconscious and apnoeic, requiring ongoing adrenaline infusion. After discussion with the gastroenterologist and the arrest team (including two ICU consultants), life support was discontinued.
There were questions over whose responsibility it was to monitor sick patients in Recovery overnight as failure to repeat ABG overnight and optimise postoperative care may have contributed to the timing of death.
Compartment syndrome
A patient suffered a post-partum haemorrhage in recovery following an elective caesarean section and was taken back to theatre for insertion of an intra-uterine balloon and vaginal pack. Post-operatively, the patient developed compartment syndrome in the left arm, requiring fasciotomies. The blood pressure cuff, ID band, and cannula were removed from the affected arm, which was elevated. The patient was unable to care for newborn twins independently and reported high pain scores.
Surgical Centres
A frail elderly patient was scheduled for elective hip replacement at a surgical cold site. The intraoperative course was uneventful. In recovery, the patient developed suspected ST-elevation myocardial infarction and was transferred to a local hospital (approximately 20 minutes away). Coronary angiography revealed Takotsubo cardiomyopathy. The patient suffered a cardiac arrest en route to ICU, and CPR was unsuccessful.
Prolonged block
A woman underwent elective caesarean section under spinal anaesthesia. The spinal had been inserted easily on the first pass and 2.6 mL 0.5% heavy bupivacaine with 300 mcg prefilled diamorphine administered.
The patient was reviewed by a consultant anaesthetist postoperatively because of prolonged motor block, and an MRI of the lumbar spine was arranged to rule out cord compression. Further imaging over the weekend included CT head and MRI head, both reported as normal. A neurology review was requested but did not occur until the following day.
Over the weekend, lower limb movement remained restricted and there was decreased sensation in L4, L5, and S1 dermatomes. Plans were made for trial without catheter and attempts to mobilise.
Risk of stroke during major cancer surgery
A patient, in their 70s, was slow to wake in PACU after a 10-hour pelvic exenteration. On extubation, the patient was unable to open their eyes or speak and appeared to have left-sided weakness. The patient was immediately taken for a CT head scan, which confirmed a stroke. Risks of major complications, including stroke, had been explained during preoperative assessment as part of consent for anaesthesia and surgery.
Underestimation of risk of high spinal based on patient characteristics
A patient was booked for elective caesarean section. Spinal anaesthesia was technically difficult due to severe obesity and resulted in a high block above T1, associated with refractory hypotension and difficulty breathing. The patient required significant doses of vasopressors, including phenylephrine, ephedrine, and metaraminol. This led to an overshoot in blood pressure, and the patient became hypertensive with a frontal headache intraoperatively. Both hypertension and headache resolved after stopping vasopressor medication.
After surgery, whilst on the ward, the patient suffered two seizures. A CT brain demonstrated a subarachnoid haemorrhage. The patient was transferred to another Hospital for further management.